COVID-19: Impact on Children in Kenya
Kenya is a high risk country for COVID-19 due to its relatively weak health system and challenging contexts (e.g. in informal settlements where self-isolation is near impossible). With the virus now spreading through communities according to the Ministry of Health, the situation could now deteriorate rapidly. We have a small window of opportunity to prevent a disaster. Save the Children is focusing on marginalized and vulnerable children – children in urban informal settlements, refugee camps and in Arid and Semi-Arid Lands (Turkana, Wajir, Mandera, Garissa) and Bungoma and Busia.Children are facing increasing protection risks due to the impact of COVID-19 in Kenya. Loss of income, loss of or ill caregivers may force many children to beg for food, take hazardous jobs to support their families, or see their families split up in search of food, leaving them alone, unprotected and exposed to violence, abuse and exploitation. Families may be forced to marry off their younger daughters to wealthier families to help relieve the financial pressures at home, exposing them to sexual abuse and early pregnancy. The situation is compounded following the Government control measures to close all schools meaning children are left without a vital safeguarding support.
Health challenges in Kenya means that many children already have serious underlying health issues;COVID-19 will only exacerbate these vulnerabilities. These children include those who have compromised immune systems due to common illnesses in Kenya like pneumonia and malaria; those who are food insecure and malnourished due to recurrent climatic shocks alongside refugees and host communities living hand to mouth.
COVID-19 must not result in us forgetting the serious health issues children already face; they must continue to receive adequate, quality care.
Children living in informal settlements in Nairobi are a key priority. Nairobi is becoming the epicentre of the COVID-19 crisis in Kenya with one of the highest informal settlements population in the world. The cramped setting with poor quality housing makes social distancing almost impossible. Most residents rely on casual labour to survive and therefore self-quarantine – staying at home for at least 14 days – is scarcely an option. Limited access to adequate water and sanitation and public health facilities will also cause a serious risk of the virus spreading rapidly.
Kenya’s health system is under resourced is ill prepared to take on wide scale medical emergency. Health workers lack comprehensive training on the management of COVID-19 as well as the correct personal preventive and protective equipment (PPE) to protect them from the disease. The sparsity public health centres hinder many families’ access adequate health care, highlighting the need for a localized, community level response to the health crisis to reach the most marginalized.
Malnutrition amongst children will increase as families have less income to meet their basic needs due to market closures and restrictions on movement. This will have dire consequences for the half a million children who are already malnourished in Kenya. Many of the poorest families are dependent on casual work and have no economic safeguards. Without an income, they will be forced to deplete whatever food, fuel and water stocks they have to get by.
OUR RESPONSE: A Child-Centred Approach
COVID-19 will have serious effects on already vulnerable children (e.g. those battling with pneumonia, malaria, malnutrition) and the knock on effects of the virus for things like education and child protection will be severe, with the impact felt for years to come.
Save the Children adopts a child-centred approach to our programming, involving children, their families and the community to best understand what will result in the biggest impact for children and keeping children safe. We are doing the same in our response to COVID-19. Key strategies include:
Communicating child-friendly age-appropriate information so that children understand and implement steps to keep themselves and their community safe from infection.
Consulting and engaging children in our response, through rapid assessments and ‘pulse checks’ with children so we can better understand and respond to their issues and they themselves can take the lead on issues affecting them.
Scaling up child protection services by building the capacity of the social service workforce, community child protection networks, and health system to ensure child abuse cases are reported and responded to, and adequate counselling and psychosocial support is provided.
Advocating with duty bearers, together with other civil society organisations and children themselves, to ensure the issues of children are considered in all stages of the COVID-19 response.
Ensuring vital lifesaving services for children do not stop. We are working creatively and innovatively to adapt programmes that will ensure lifesaving services continue for the most marginalised children. This will help mitigate adverse effects of the COVID-19 virus on children.
OUR RESPONSE: What We’re Doing Overall To Tackle COVID-19
Risk communication and community engagement
Providing age-appropriate integrated health, hygiene, and child protection information messaging to the communities through mass media, information materials, and through our existing community networks to counter misinformation and mitigate the risks related to COVID-19.
Establish a two-way dialogue with community members at all levels (including children youth and women) that seeks to understand their perspectives, solicits their inputs, shares information, explain their fears, ask questions (and have them answered), and engages them in the response.
Health and Nutrition:
Training & equipping our extensive network of health workers via online platforms with the information and tools necessary to diagnose and treat COVID-19 infections, whilst also developing strategies to protect them from infection such as providing protective wear and developing guidelines for virtual trainings.
Maintaining life-saving nutrition and health programming throughout the crisis making adaptions where needed in the face of COVID-19.
Provide child friendly isolation kits in coordination with the MOH that includes toys and readers to keep children occupied if they have to be quarantined or in isolation.
Health and Nutrition:
Training & equipping our extensive network of health workers via online platforms with the information and tools necessary to diagnose and treat COVID-19 infections, whilst also developing strategies to protect them from infection such as providing protective wear and developing guidelines for virtual trainings.
Maintaining life-saving nutrition and health programming throughout the crisis making adaptions where needed in the face of COVID-19.
Provide child friendly isolation kits in coordination with the MOH that includes toys and readers to keep children occupied if they have to be quarantined or in isolation.
Water, sanitation, and hygiene:
Distributing soap, hand sanitizers and handwashing facilities to communities. Priority will be given to families living in informal settlements and refugee camps due to limited access to safe water and sanitation facilities
Ensuring safe water supplies are accessible within communities where possible – particularly in health facilities, as well as schools in the recovery period. Household water treatment will be provided so families can treat and disinfect their water.
Child Protection and Education:
Provide psychosocial support and respond to violence and abuse of children by supporting Government child protection reporting platforms and social service workforce.
Support distance learning by sensitizing families on the available radio lessons – or providing radios where necessary for continued learning, particularly in Dadaab refugee camp in non-formal schools.
Lead back to school campaigns when the worst is over to make sure that the most vulnerable children return to, and stay in school.
Food Security and Livelihoods:
Using multi-purpose cash transfers (through mobile means where possible) to provide a safety net for the most vulnerable families.
Engaging and motivating youth groups to make soap, masks, sanitizer that can support the emergency response and provide an income
Monitoring of market dynamics to inform the response, working in coordination with the National Drought Management Authority (NDMA) and through telephone calls with traders and consumers – our field staff in Turkana, Mandera, Wajir, Garissa, and Nairobi already have a relationship with these key informants.
Save the Children: Positioned to Tackle COVID-19
Global Movement: Active for over 100 years we are the world’s biggest independent NGO. We’re active across Kenya, from Nairobi to Turkana focussing on ensuring every single child survives, learns and is protected. We focus especially on vulnerable girls who often need our help the most.
Leading health actor: Save the Children is recognized as a leading actor for neonatal, newborn, maternal and child health in Kenya. We enhance Government health systems and improve their existing
structures to scale up successful programs. This approach has enabled us to establish excellent relationships with the national and county government and achieve sustainable impact at scale.
Innovation: Kenya is a key country for new technology and ICT innovations across the continent. Recognising this, Save the Children’s global ICT hub is hosted in Kenya. The Kenya country office has worked with the ICT hub to embed number of innovative technological solutions within it programming, for example e-training platforms for health workers. We will build on these innovations during the response to continue to deliver services for children innovatively in light of COVID-19 restrictions.
Reach: In 2019 our life-saving and life-transforming work directly impacted the lives of 1,311,524 people, 923,339 of whom were children.But that’s not the whole picture, the knock-on effects of our programming had an impact on more than 2.2 million people in Kenya in 2018.
Connected: We are a trusted voice with the likes of the Ministry of Health, the Kenyan UN Cluster System and fellow NGOs. Our advocacy teams work closely with key national change makers to deliver for children: influencing legislation, budgets and government systems. Recently our efforts resulted in a Community Health Service Bill to remunerate community health volunteers in Turkana county and a 5.8% increase in Bungoma’s health budget.
Experienced: We played a leading role all the recent major health crisis in Kenya, including the ongoing locust invasion. We responded to a Measles outbreak through a mass vaccination campaign in Wajir county, and a cholera outbreak in Mandera that reached 9,118 people last year. We have the experience, expertise and lessons learned to have a significant impact in the fight against COVID-19.
Community Acceptance: Our work is grounded in community acceptance where we collaborate with existing representative bodies and networks making sure our impact is sustainable. We have a long-standing presence in some of the most under-resourced parts of the country including: Nairobi informal settlements, Turkana, Wajir, Mandera, Garissa, Bungoma and Busia. Our historical relationships mean we have a deep understanding of the communities we serve in these counties, their sociocultural issues, and county government structures. Where restrictions mean we can’t be there in person, these relationships will be vital.
Emergency Health Teams:We have deployed our global specialist emergency teams to Kenya to provide extra capacity to respond to this virus. Already we are liaising with the Ministry of Health to find out how we can best leverage these teams to support the response.
By Delfhin Mugo and Florence Dzame
Learning remains paralysed across the country due to the coronavirus pandemic, yet, for most children, education is the key to a brighter future. The situation is even worse for refugee children, most of whom begin school late, and for whom education is also the only hope out of the camps.
At the Daadab Refugee Camp in Northern Kenya, a local radio station, Gargar FM, is giving hope to children seeking an education.
“Young learners, especially those in the refugee camp, are more affected since they cannot access digital learning tools. Also affected are learners with special needs who cannot follow radio lessons,” said Mr Tukow Nuuh, a programme manager with Save the Children.
GREATEST DISRUPTION
Children in Kenya are facing the greatest disruption to their education after schools were closed indefinitely nearly two months ago.
The Ministry of Education estimates that 16,528,313 learners are out of school, from early childhood development education to secondary school students.
But the situation in the camp is much worse. Here, at least 50 per cent the population comprises children, and more than 40,000 school-age children were already out of school, data from the United Nations High Commissioner for Refugees and the Education Management Information System, respectively, show.
In a bid to keep the children learning, children’s welfare organisations, including Save the Children and UNHCR, are using the radio station to broadcast lessons to students.
But because most children at the camp are late starters, the education offered is non-formal, a crash course of sorts to help the students catch up with their peers. Different subjects are taught via the station for an hour twice a week, including maths, English, environmental studies, religious education and creative art.
“This is crucial in ensuring that they do not lag too far behind,” Mr Nuuh said.
A survey showed that about 60 per cent of the learners have radios and can tune in.
CREATES AWARENESS
The programme also creates awareness about Covid-19 preventive measures and the channels for reporting suspected cases to the authorities.
The aid agencies have appealed to the Ministry of Education to urgently ensure that systems for remote learning are in place, as the most marginalised children have been hit hardest by the closure of schools.
Save the Children says priority should be given to children who cannot access digital learning tools - those from low-income households and in rural and marginalised areas, those with disabilities, and those in refugee camps.
“It will cost more if we don’t act now. We know from other public health crises that once older children lose access to education, they are less likely to return. This is also the case with the most vulnerable children, who end up in child labour, child marriage and facing other life-threatening situations,” Save the Children Director for Kenya and Madagascar Wang Le told the Nation.
“For younger children, even a few months of missed education can have long-term effects, requiring additional and intensive remedial efforts to catch up.”
Ms Le said other measures to help the children include supporting distance learning by making families aware of the radio lessons being offered by the Kenya Institute of Curriculum Development for formal learners, and supporting the recording of lessons for non-formal learners. The organisation is also working towards providing radios where necessary for continued learning, particularly in refugee camps, Nairobi’s informal settlements and arid and semi-arid counties in Northern Kenya.
“We are also providing remote counselling and psychosocial support for children and sensitising communities via mass media about the increased risks for children and how to protect themselves during the pandemic,” she added.
We will be leading back to school campaigns when the worst is over to make sure that the most vulnerable children return to, and stay in school,” said Wang Le.
This article was first published on the Daily Nation on May 20, 2020

By Florence Dzame
In Daadab Refugee Camp in Northern Kenya, young learners tune into Gargar radio to participate in education sessions supported by Save the Children. Children in Kenya and across the region are facing the greatest disruption to their education in living memory due to closure of schools as a measure to prevent the further spread of COVID-19. Since the directive was issued by the Ministry of Education for schools to close by 20th of March 2020, an estimated 16,528,313 learners in Kenya are out of school according to the National Education Sector Plan (2019-2023, from Early Childhood Development Education to Secondary school learners. The situation in the camp is even direr because 50% of the camp’s population are children and more than 40,000 school-age children were already out of school according to UNHCR and Education Management of Information System data.
“Young learners especially those in the refugee camp are more affected since they cannot access digital learning tools. Also affected are learners with special needs and impairments who cannot follow through radio lessons,” said Tukow Nuuh Program Manager Save the Children
Save the Children, other implementing partners and other UNCHR departments came together to ensure learners in the camp enrolled in non-formal education continue to access education during the pandemic. The radio sessions air different subjects (including mathematics, english, environment, religious, education and creative art) twice a week for one hour using the non-formal curriculum. The programs are live and the teachers go to the radio stations to deliver the lessons.
Radio Presenter in Daadab Refugee Camp during the education programs
Reports show that about 60% of the learners have radios and are able to tune in.
The programs also create awareness on COVID-19 prevention measures and reporting channels of suspected cases to the authorities.
Save the Children calls for the Ministry of Education to urgently ensure that systems for inclusive remote learning are in place, recognizing school closures will hit the most marginalized children hardest. Particular priority should be given to children who cannot access digital learning tools. These are children from low-income households, rural and marginalized areas, those with disabilities and children from the refugee camps.
“It will cost more if we don’t act now. We know from other public health crises, that once older children lose access to education, they are less likely to return. This is also the case for the most vulnerable children, who end up in child labour, child marriage and facing other life threatening protection risks. For younger children, even a few months of missed education can have long-term effects on their lifelong learning, requiring additional and intensive remedial efforts to catch up,” said Wang Le, Country Director Save the Children Country Kenya and Madagascar
Since the start of the outbreak, Save the Children continues to respond to the needs of communities in countries impacted by the COVID-19 outbreak. We are supporting distance learning by sensitizing families on the available radio lessons being offered by the Kenya Institute of Curriculum Development for formal learners and supporting recording of lessons for non-formal learners and working towards providing radios where necessary for continued learning, particularly in Daadab refugee camp in non-formal schools, Nairobi informal settlements and Arid and Semi-Arid counties in Northern Kenya. We are also providing remote counselling and psychosocial support for children and sensitizing communities via mass media on the increased risks for children and how to protect themselves during this pandemic. We will be leading back to school campaigns when the worst is over to make sure that the most vulnerable children return to, and stay in school.

By Florence Dzame
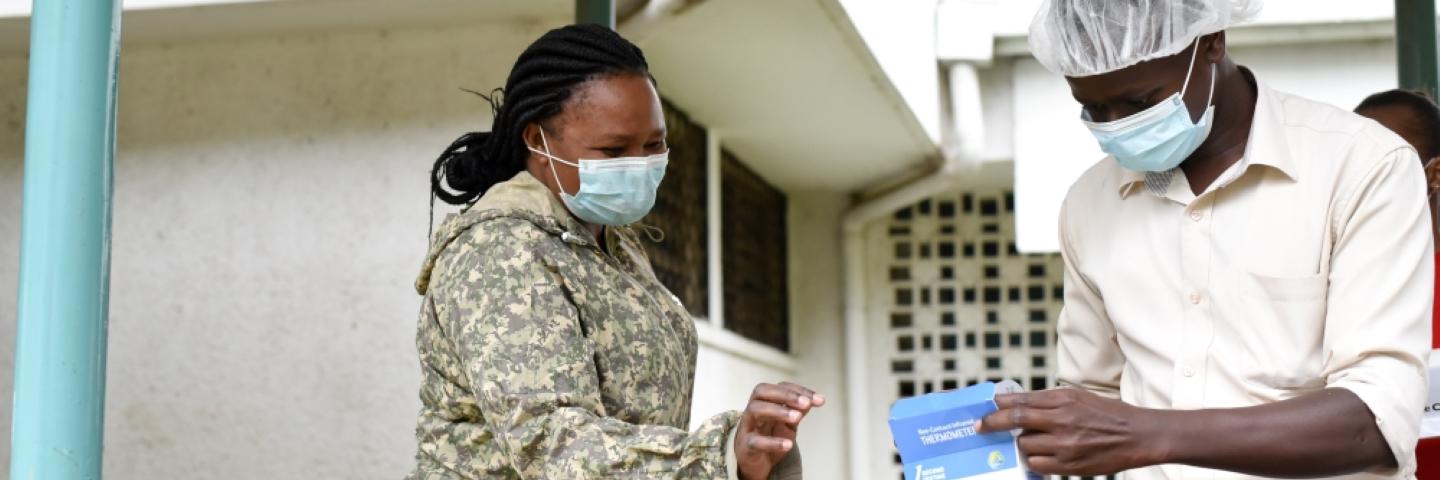
In Kibra the largest urban slum in Nairobi and also Africa, Domtilla Ogaro, 49, receives a consignment of infection and disease prevention control items from Save the Children. Ogaro is the sub county clinical officer with 24 years of experience as a health worker. Most of Kibra slum residents live in extreme poverty, earning less than $1.00 per day. A great majority of the people living in this slum lack access to basic services, including electricity, running water, and medical care. As cases of COVID-19 continue to rise in the country, a big source of concern is how it will spread and affect those that live in congested low-income areas. Save the Children has mobilized quickly to alleviate the impact of COVID-19 in informal settlements of Kibra and Mathare slums in Nairobi.
“We are distributing infection and prevention control items like gloves, handwashing stations, masks, hand sanitizers. We are conducting trainings for health care workers and supporting messages on community radio to help prevent the spread of COVID-19,” said Ken Kagunda Program Manager Save the Children.
So far in Kibra slums we have distributed 25 hand washing equipment, 50 bar soaps, 37 five liter jerry cans of soap, 13 boxes (50 pieces each) of surgical masks, and 13 googles with support from various donors.
“The community here needs a lot of sensitization since there is a lot of misinformation and stigma. They also need more handwashing facilities and masks since the population is large and they are very congested. Not everyone is able to afford masks since poverty levels are high, said Ogaro.
Francis Odera, 40, a Community Health Volunteer (CHV) from the area confirms Ogaro’s remarks. He has worked as a CHV for 10 years and is a father of six children.
“The community needs more sensitization because there is a lot of fear. Some community members don’t understand COVID-19 at all and only put on masks to avoid arrest by the police,” he said.
By 20 May, 963 cases have been confirmed in the country and the government has intensified mass testing in targeted areas, including on enhancing screening along border points. The Government has also restricted across the Kenya- Tanzania & Kenya - Somalia border.
Save the Children is responding to COVID-19 through programmatic interventions that support risk communication and community engagement, health and nutrition, water sanitation and hygiene (WASH), child protection and education and food security and livelihood for vulnerable children and families.

Thursday, 30 April, 2020
FOR IMMEDIATE RELEASE
Children in Kenya are facing the greatest disruption to their education in living memory due to closure of schools as a measure to prevent further the spread of COVID-19, says Save the Children. Since the directive was issued by the Ministry of Education for schools to close by 20th of March 2020, an estimated 16,528,313[1] learners in Kenya are out of school, from Early Childhood Development Education to Secondary school learners.
Besides offering a critical pathway to employment and supporting children to become productive and informed citizens, education also plays a critical role in keeping children protected through a safe and consistent place to stay while their parents are at work, nutrition in the form of school meals, and where necessary ensuring vulnerable families have access to more specialized services like psycho social counselling, assessment and possible referral for specialized interventions
The closure of schools is not only preventing children from learning and enjoying all the other benefits that education provides, but it is also exposing children to increased risks of abuse, neglect, child labour, and human trafficking. The closure of schools and containment measures means children are confined in spaces with possible perpetrators. Reports have shown that parents are the most common perpetrators of violence against children[2]. Girls are more likely to drop out of school completely since they face a disproportionately larger burden for caring for family members who contract the virus, and taking care of younger children while their parents seek work. Girls are also at greater risk than boys of negative family coping mechanisms increased risk of sexual exploitation, early and unintended pregnancy, and child, early and forced marriage. In this crisis, Save the Children has noted the profound effects on the psychosocial well-being of children and youth, especially when the routine of schooling and the sense of normalcy that this routine provides were disrupted.
Save the Children calls for the Ministry of Education to urgently ensure that systems for inclusive remote learning are in place, recognizing school closures will hit the most marginalized children hardest. It’s also vital that local and the national government supports and equips teachers with the skills to provide quality distance teaching.
Particular priority should be given to children who cannot access digital learning tools. These are children from low-income households, rural and marginalized areas, those with disabilities and children from the refugee camps.
Wang Le, Country Director Save the Children Country Kenya and Madagascar said:
“It will cost more if we don’t act now. We know from other public health crises, that once older children lose access to education, they are less likely to return. This is also the case for the most vulnerable children, who end up in child labour, child marriage and facing other life threatening protection risks. For younger children, even a few months of missed education can have long-term effects on their lifelong learning, requiring additional and intensive remedial efforts to catch up.”
Since the start of the outbreak, Save the Children continues to respond to the needs of communities in countries impacted by the COVID-19 outbreak. We are supporting distance learning by sensitizing families on the available radio lessons being offered by the Kenya Institute of Curriculum Development and working towards providing radios where necessary for continued learning, particularly in Dadaab refugee camp in non-formal schools, Nairobi informal settlements and Arid and Semi-Arid counties in Northern Kenya. We are also providing remote counselling and psychosocial support for children and sensitizing communities via mass media on the increased risks for children and how to protect themselves during this pandemic. We will be leading back to school campaigns when the worst is over to make sure that the most vulnerable children return to, and stay in school.
About Save the Children
Save the Children has been providing support to children in Kenya through our development and humanitarian programmes since 1950. We work with communities, local partners, and the government to design and deliver programmes to meet the needs of the most deprived children. We also advocate for greater investment of public and private resources for children.
[1] National Education Sector Plan (2019-2023)
[2] According to the Violence Against Children (VAC) 2010 report and findings of National Council for Children Services (NCCS) and Kenya National Bureau of Statistics (KNBS) assessment 2014, indicate that parents were the most common perpetrators of violence against children, closely followed by teachers and religious leaders, and other people unknown to them|
###
Media Contact
Florence Dzame
Communications and Campaigns Manager
Mobile 0723435245

By Marion Kwambai
Godfrey Eimun, 42, lives in Turkana County Northern Kenya with his wife and eight children. He works at the Chief’s office and also chairs the community water and farming committees. His community has about 4,360 people whose main form of livelihood is farming through canal irrigation from River Turkwel.
Eimun said he first heard about COVID-19 in December last year when it was first reported in Wuhan. He heard about it on radio and has been following the news until he heard that the virus is now in Kenya.
“We are just recovering from a prolonged drought, in most households the food situation is still not stable and this pandemic has brought a lot of fear amongst us and uncertainty in our livelihoods. It is threatening our survival especially that of our children,” said Eimun.
Chronic marginalisation has left Turkana with a dearth of basic services. The pandemic can be further aggravated by pre-existing issues in the county such as limited access to health and nutrition service, poor childcare practices, high illiteracy and poverty.
“Our children have no means of alternative learning since the Government directed all schools to be closed and children stay at home either playing and helping out with house chores. We are also worried about their food security since markets have been closed and we are not able to sell our animals to get money for food,” he said.
He fears that once they have completed the food stock they currently have then they will not know what to do.

Save the Children together with the County Government of Turkana has been conducting community outreaches and house to house visits to create awareness on COVID-19.
“We are distributing hand sanitizers, disinfectants, and soap and handwashing stations in the county. We have rehabilitated boreholes for communities to access safe water and have also supported health facilities receive water in Kibish and Turkana sub counties. We are supporting cash transfers to households with malnourished children in Turkana North to cushion families from the impact the pandemic has had on markets and food supplies,” said Bernard Ekidor, Save the Children Emergency Response Coordinator.
Eimun said that he now has to cope with the new way of life that has changed since the pandemic started.
“All social gatherings such as weddings have been cancelled, barazas, markets and animal auctions have been closed,” he said
So far there have been no cases reported in Turkana County. The Ministry of health has set up an isolation centre at the Lodwar County Referral Hospital to combat the pandemic.
So far, the country has reported 374 confirmed cases of COVID-19 across the country.


By Wang Le Country Director Kenya and Madagascar
Children face multi-dimensional risks during infectious disease outbreaks. These include exposure to infection and indirect risks to their right to education and healthcare from policies implemented to reduce contamination and direct risks to their care and protection.
While current trends indicate that children are not among the most vulnerable group, more data is urgently needed to understand the nature of transmission and vulnerability of children to Covid-19.
The coronavirus is likely to have devastating effects to children, especially the poor and marginalised ones. There is evidence that the virus will have serious effects on already vulnerable children — including those battling pneumonia, malaria or malnutrition.
National healthcare systems are pivoting to respond to the outbreak while also still guaranteeing access to essential quality services that are critical for child survival. However, children’s health is often compromised as a result of reduced access to healthcare services, including disruption of routine immunisation and antenatal care, due to intense pressure on healthcare systems.
Other effects of the pandemic include severing children’s access to education and protection. With schools closed, there is a risk of increased cases of child abuse, violence and exploitation, even by parents and people known to them.
Those who rely on the school feeding programme will miss a meal or go hungry. For many children, these meals must now be provided at home, by caregivers who are already stretched financially.
Then there is interruption of children’s safe and appropriate care due to the absence or loss of primary caregivers, which also negatively affects their mental health and well-being.
Also, children already growing up in extremely difficult contexts just got another burden to cope with. Those outside of family care — including among street families, in institutions or detention and refugee camps — are particularly vulnerable, including to discrimination within the community.
Besides, millions of refugee children and displaced families, who live in overcrowded, often unhygienic areas with limited access to medical care, will not be in a position to isolate or distance themselves from others or comply with basic hygiene, including handwashing.
We must think about rapidly scaling up support to these vulnerable groups and providing the social protection that they urgently need. The poorest households — including those suddenly impoverished by this crisis and those who live on daily wages — will need support to survive this shock and ensure their most vulnerable members, children, are protected.
The lessons from this crisis will be many and far-reaching. We must continue supporting communities with information on how to stay safe and prevent the spread of infection. We must also adapt to responding to the new needs this creates and be prepared to respond in vulnerable communities that will be hardest hit in the coming period to efficiently and effectively safeguard the most vulnerable, including children.
This article was first published on the Daily Nation on April 13, 2020.

Save the Children has been operational in Kenya since the 1950s, providing support to children through developmental and humanitarian relief programs delivered both directly and through local partners. Current programming focuses on child protection, child rights governance, education, health, HIV/AIDS, livelihoods, nutrition and WASH. In 2012, as part of a global reorganization process. We are the largest global independent organisation for children.
It is trite that Covid-19 is a global pandemic, which threatens children’s rights in countries around the world and exposes them to potential disruption to their education, healthcare, protection and wellbeing, including social interaction with family members, teachers and adult caregivers. Granted, children have been grossly affected with one death so far reported and a number still recovering after diagnosis. We have witnessed an increase in sexual violence cases, with children being affected.
Save the Children’s previous experience of responding to infectious disease outbreaks highlight major risks to children and their families that arise from the pressure on healthcare systems resulting in reduced access to routine health services (e.g. disruption of routine immunisation and antenatal care services). Further impacts include heightened exposure to child protection risks of neglect, abandonment, violence and exploitation through loss of or separation from primary caregivers. Children living and working on the streets those in care homes, juvenile justice and other detention centres are extremely vulnerable to infection. Cumulatively, there is an exacerbation of gender-based violence with profound psychosocial impact that may arise from the existing curfew, quarantine, isolation, stigmatisation and separation from or loss of caregivers.
As a multi-mandated organisation, we have identified serious concerns about the immediate and long-term impact Covid-19 and the ongoing response measures may have on the health and well-being of children, especially those most vulnerable.
Our five overarching concerns for children are:
1. Challenges on access to routine basic health services;
2. Increased child protection risks;
3. Disruption to education;
4. Lost family income/livelihoods and resultant food insecurity; and
5. Potential economic slowdown
To address these concerns, it is critical for this Honorable House to make proposals on an integrated approach that prioritises the needs and rights of children, especially those most vulnerable, and mitigates the long-term impact this pandemic may have on them, their families, and their communities, today and for years to come.
1. Challenges on access to basic health services
It is important to note that whereas the country’s healthcare systems are already responding to the pandemic, outbreak, the same system is expected to continue discharging its expectation of guaranteeing access to essential quality health services that are critical for child survival. However, our experience of responding to infectious disease outbreaks tells us that children’s health is often compromised during such responses with services such as routine immunization and antenatal care services being relegated to the back banner due to intense pressure on national healthcare systems. We are particularly concerned about reports of mothers who have been unable to access health care services during this difficult times. A case in point was reported in the Standard Newspaper (7th April 2020), where Catherine Twili from Mutei Village in Mbooni, delivered her baby alone, and she did not wake up the following day, she was found dead, the new born next to her. The baby survived. Kenya stands the risk of reversing the gains we had begun making on reducing maternal mortality and ending preventable deaths of new borns and children under the age of five years.
Health workers are very critical during this period. We have witnessed isolated cases of health workers threatening to “down their tools” after raising concerns over remuneration and failure to be provided with the requisite protective equipment necessary for the discharge of their duties. It is unfortunate to note that scores of health workers are reported to have contracted Covid-19 in line of their duty.
Noteworthy, children experiencing community and household quarantines, the loss of family members and friends, and increasing deprivations due to social disruption may experience psychosocial trauma. Caregivers experiencing significant stress may not provide appropriate care and protection for their children. Finally, children whose caregivers succumb to the virus, or whose families’ livelihoods are disrupted, will be more vulnerable to violence and exploitation.
It is in this regard that we appeal to this Honorable House in exercise of its oversight mandate as stipulated under Article 96(3) to Ensure that the provision of these routine child health care services is not compromised during this period.
Ensure that health workers, and community health volunteers, where possible are remunerated, empowered and supported. They must also have the right training, skills, equipment, resources and supplies (including personal protective equipment) to respond and stop COVID-19 in its tracks.
2. Increased child protection risks
We have significant concerns that the spread of COVID-19 and related response measures will drastically increase protection risks for children, in existing humanitarian crises, and for children already experiencing extreme poverty. This can increase girls’ and boys’ exposure to physical and gender-based violence, child labour, child marriage, and sexual exploitation and abuse. Stigmatisation also increases the risks of physical and emotional maltreatment, social exclusion, and distress for children.
Lost income/livelihoods, food insecurity, and closure of schools and day care centres will increase family stress and conflicts within the home. Especially where traditional gender norms are strong, this may lead
to increased domestic violence and children’s exposure to greater levels of psychological, physical, and sexual violence at home.
Hardships related to the loss of income/livelihoods may also push children and families to take up negative coping mechanisms, which increase girls’ and boys’ exposure to family separation, child marriage, child labour, and sexual exploitation and abuse.
Children without parental care—whether pre-existing such as living on the streets in urban slums or consequent of a parent’s/caregiver’s death, hospitalisation or quarantine—are especially in need of protection as they lack the means to survive in a crisis, can become targets for violence and exploitation, and may not receive timely information to protect themselves from the disease. Strains on public services during a pandemic can also result in the breakdown of referrals between health and child protection systems, and the weakening of child protection services.
Children who have lost or at risk of losing parental care are under great risk and danger during the COVID- 19 crisis. This is due to challenges such as lack of access to adequate basic needs, increased cases of abuse and inadequate support to families and communities to provide for their children. There is need to ensure that the safety and protection of children in alternative care in not compromised.
We call upon this House to take a particular interest in emerging reports on violence against children, and in particular ensure that adequate resources are allocated to the Department of Children Services and the National Council for Children Services to popularise the National Helpline Toll free line 116 as a reporting mechanism for any violations of child rights.
The National Council for Children Services and the Area Advisory Councils at the county and location level are revitalised and utilized as a follow up mechanisms for such cases.
3. Disruption to education
The impact of school closure extends beyond disruption to education and carries multiple, secondary risks to children from low-income households because children may rely on school meals to support their daily nutrition intake and access protection services through school. There is overwhelming evidence that the longer children are out of school, the risk of them never returning increases significantly. We applaud the Kenya Institute of Curriculum Development and the Kenya Broadcasting Corporation for the ongoing interactive radio instruction. However, we call upon Senate to ensure that the Government puts in place easy-to-use distance learning tools, ensuring technologies used do not exclude the poor, disabled or marginalised girls and boys.
Parliament develops policies that require other private media houses, particularly community radio stations to consider engaging learners using their media houses during this period.
The Ministry of Education is challenged to think about innovative solutions for the most poor and vulnerable children.
4. Lost Family Income/Livelihoods & Food Insecurity
Covid-19 impacts essential livelihoods programmes/activities. As markets close and income generating opportunities shrink, those most vulnerable in savings groups will have even less or no income, affecting their ability to save and repay loans either to savings group or microfinance institution. Those who live in slums and depend on informal markets and daily wages for income will not be able to trade for income due to movement restrictions. In the most fragile contexts, households do not have reserves to support themselves, forcing many families to rely on external aid in order to survive.
Disruptions, including movement restrictions, are also likely to compromise parents and caregivers’ ability to make a living and meet their families’ basic needs, particular impacting women. COVID-19 will take away resources that women need, as their burden of care increases and their paid livelihoods suffer losses.
Whereas we applaud the appropriation of an additional Ksh 10 Billion to the elderly, orphans and other vulnerable members of our society to cushion them from the adverse economic effects of the Covid-19 pandemic. We ask that Non State actors that have been involved in cash transfer programmes especially in “hard to reach areas” should be involved to support the scale up the interventions during this pandemic.
Further, the Senate, in upholding its mandate under Article 96 of the Constitution should ensure that County Governments make allocations to respond to this crisis.
We appeal to Parliament to consider enacting a substantive legislation that will comprehensively address issues of Covid-19 as opposed to the current approach where Regulations are developed. Such a legislation will deal with emerging issues in a holistic manner, and will avail Parliament an opportunity to robustly engage with the Covid-19 response. The proposed stimuli programmes, health interventions and the attendant institutional frameworks will derive their legitimacy and existence from the proposed legislation.
5. Potential economic slow down
It is already evident that the pandemic will have a negative impact on the economy as income earning sectors in Kenya including tourism, manufacturing and agriculture have been severely affected due to shutdowns in major markets and the disruption of the global supply chain. It is worth noting that the three sectors accounted to over 40% of Kenya’s Gross Domestic Product (GDP) in 2018. The proposed tax cutting measures meant to cushion the populace from the vagaries of the pandemic, will cumulatively slow down domestic resource moblisation efforts by the Kenya Revenue Authority, thus resulting to a smaller resource envelop for the Government. Overall, the country’s GDP could be affected downwards by 10 to 25%.
We urge Parliament to work very closely with the Treasury on at least three fronts.
First, the Government should explore the possibility of re-negotiating bilateral loans that are due to be paid this year to be paid in the medium term, thus freeing the much needed resources to address the on-going pandemic. This is in tandem with
The World Bank and the International Monetary Fund (IMF) plea on international bilateral creditors to suspend debt payments to give developing countries including Kenya time to absorb shocks of coronavirus pandemic.
Secondly. This House should urge the Treasury to robustly engage bilateral creditors on the need to waive interest on the debts due. According to UNCTAD, such a waiver will avail USD 44 Billion to African countries, including Kenya, which will certainly go a long way in helping African Governments to mitigate the effects of Covid-19.
Finally, this House should unanimously support sections of the international community, that are spearheading calls for debt cancellation. Writing off developing country debts, based on need rather than bargaining power, is very critical. UNCTAD has been unequivocal on this by noting that “…the wall of debt repayments about to hit a large number of developing countries is unsustainable.”
CONCLUSION
Save the Children is grateful for the opportunity availed by this Honourable House present this memorandum for and on behalf of Kenyan children and reassures all children, parents, caregivers, the Government of Kenya and other stakeholders of its unwavering commitment to be involved in both preventive and response initiatives as shall be practically possible. We are available to offer any clarifications on this memorandum, and welcome an opportunity to make an oral presentation upon request. Together we shall overcome the threats of COVID-19.
Signed by ………………………………………………………………….
Wang Le, Country Director
or more information, please contact
Ibrahim Alubala, Child Rights Governance and Advocacy Technical Specialist,
Save the Children, Kenya Country Office
Email: Ibrahim.alubala@savethechildren.org
Tel No. +254722378582

By Florence Dzame
In far flung communities in Turkana County, Northern Kenya Save the Children and officials from the Ministry of Health are moving from door to educating members of the community on COVID-19. They are conducting sensitizations in communities that are far from health facilities. In the county it is an average distance of at least 30 KMS to the nearest health facility. COVID – 19 is global pandemic that will have far-reaching impacts on children, not only on health outcomes, but also on education, protection, nutrition, food supplies, and livelihood. The pandemic can be further aggravated by pre-existing issues in the county such as limited access to health and nutrition service, poor childcare practices, high illiteracy and poverty.
Benjamin Eleyo, 27, a community mobilizer with Save the Children said that they are able to cover 40 houses in a day.
“We give nutrition commodities and soap as we move from house to house,” said Eleyo.
Another approach that Save the Children is using to create awareness about this pandemic is to conduct education sessions during the integrated health outreaches. The outreaches are held bi-weekly.
“We teach community members about how the virus is transmitted, proper-handwashing and social distancing,” said Eleyo.
So far there have been no cases reported in Turkana county. Kenya has recorded the highest jump in coronavirus cases so far, with 22 people testing positive Wednesday. This brings the national total to 81.


March 23 – Governments and communities must act now to ensure that millions of vulnerable children do not lose out on their education as schools close their gates to try and contain the Coronavirus outbreak, warns Save the Children.
More than 120 countries have already introduced nation-wide school and university closures affecting nearly three-quarters of the world’s student population – an estimated 1.2 billion learners – according to UNESCO. That number is expected to rise as the Coronavirus looks set to spread further.
Save the Children calls on governments to urgently ensure appropriate care is available to children along with inclusive remote learning, recognizing school closures will hit the most marginalized children hardest. It’s also vital that governments support teachers and equip them with the skills to provide quality distance teaching.
The impact of school closures extends beyond disruption to education – they also carry other risks to marginalised children and children from low-income households, because many may rely on school meals to support their daily nutrition.
Gabriella Waaijman, Save the Children’s Global Humanitarian Director, said:
“We are facing an unprecedented situation. The number of children suddenly out of school or university is equivalent to the entire population of India. Hundreds of millions of students won’t be able to return to normal classes for months, possibly longer, with many important exams postponed or cancelled altogether.
“We know from experience that the longer children are out of school, the more likely it is they will never return, especially girls and those from low-income households. That’s why governments must put in place easy-to-use distance learning tools now, ensuring the technologies used aren’t excluding poor, disabled or marginalised children. We need to get creative. In communities with little or no access to the internet for example, radio programs can enable children to continue their learning.
“Now is the time for the world to pull together to protect the most at-risk children around the world, who are going to be hardest hit by this global crisis. These include homeless children, children in care and children who may be living alone without parents or caregivers. Disabled children may be further isolated or neglected if they can’t go to school while refugee and displaced children in temporary camps are even more vulnerable than they were before this crisis.”
“As pressures mount on low income families, children may need to work to bolster family incomes, and girls especially may also face a disproportionate burden of caring for family members who contract the virus or taking care of younger children. If plans are not put in place urgently, some children run the risk of never returning to school at all.”
For more information contact the Country Director Kenya and Madagascar Ms Wang Le on Le.Wang@savethechildren.org and National Health Focal Person / Save the Children Head of Health and Nutrition Dr Lynn Kanyuuru on Lynn.Kanyuuru@savethechildren.org

By Inger Ashing CEO of Save the Children
“There are 415 million children living in conflict - they are dying from violence, recruited and abducted, detained and abused. Now they face the added risk of losing loved ones to the virus or being infected themselves. It is impossible to properly fight such a pandemic when bombs are falling, or go to a hospital when bullets are flying. You can’t scale up much needed health services when soldiers are fighting in the streets.”
Covid-19 attacks families everywhere indiscriminately and is set to wreak havoc on millions of children’s lives. Save the Children fully supports the call of the Secretary General who today called for a global ceasefire to be enacted immediately, to help protect children in conflict from further danger.
We now need to support countries that have been ravaged by war for years. Countries where the health systems are already at breaking point – they need time to prepare themselves as best as they can for what might be coming. A stop to the fighting will give them that space. The world needs to come together in humanity at this moment, and that’s not possible in places where war is raging.”
For more information contact the Communication and Campaigns Manager Ms Florence Dzame on Florence.Dzame@savethechildren.org.

By Kevin Watkins Chief Executive Save the Children UK
The coronavirus crisis is providing a tough reminder of the wisdom behind Benjamin Franklin’s adage that “an ounce of prevention is worth a pound of cure”. But as governments in Europe and the US pump billions of dollars into overstretched health systems, and trillions into economic support, Africa is drifting towards a human catastrophe that could dwarf what we have seen in Europe and North America — and the world is watching.
Perhaps the complacency comes from the headline reported numbers. On Thursday, sub-Saharan Africa recorded its first Covid-19 death — the vicepresident of Burkina Faso’s legislative assembly. The whole region has reported just 279 confirmed cases — less than 1 per cent of the world total. Only South Africa, Senegal and Burkina Faso have more than 20 confirmed cases.
But the warning signs are flashing. Confirmed cases have increased three-fold over the past week. While most of the early cases were imported by visitors from Europe, seven countries have now reported community transmission, including Kenya, the Democratic Republic of Congo and Liberia. Moreover, whatever the headline numbers they almost certainly represent the tip of a very large iceberg because testing is limited.
Tedros Adhanom Ghebreyesus, the director-general of the World Health Organization, has called on African leaders and the international community to “wake up” to the threat facing the region. They should listen. If we have learnt nothing else from the crisis it is that advice from the WHO should be taken seriously. Yet, with western governments focused on their own countries, the sleepwalking continues.
It is impossible to overstate the scale of the threat now facing Africa. The region’s health systems are woefully ill-equipped to deal with current challenges, let alone a coronavirus pandemic. According to the WHO, the region has a shortage of 3.6m health workers. Half of the population has no access to modern health services. Covid-19 kills through viral pneumonia. The fact that more than 400,000 African children die each year from pneumonia because they are denied access to basic healthcare speaks volumes about the region’s ability to respond to the coming crisis.
Comparisons with rich countries should be amplifying the WHO’s wake-up call. Health services across Europe are buckling under the strain of the coronavirus response. With one of Europe’s most developed health systems, Italy has 41 doctors for every 10,000 people. Senegal, now in the early stages of a possible coronavirus epidemic, has fewer than one doctor for every 10,000 people.
These comparisons tell only part of the story. Last month, as part of a Save the Children mission, I visited health clinics and hospitals in Jigawa state, in northern Nigeria. Medical oxygen was conspicuous by its absence. In one hospital, there was one small concentrator for an intensive care ward treating 30 children. Sadly, that is not unusual. The absence of medical oxygen helps explain why pneumonia is the biggest killer of Nigeria’s children — and it’s what threatens potential Covid-19 victims.
Speculative “expert” commentary has fuelled international complacency. Africa has been protected, runs one argument, because warm weather limits Covid-19 transmission. But high transmission rates in the Philippines and Florida tell a different story. Others point to a supposed “demographic advantage”. Africa, according to the theory, has more (less susceptible) children and fewer vulnerable elderly people But what about children whose immune systems are weakened by elderly people. But what about children whose immune systems are weakened by malnutrition, malaria and diarrhoea?
We are living in Europe with the consequences of a catastrophic failure in international co-operation to prevent what was a containable epidemic mutating into a global pandemic. Delayed and disjointed national action has proven a weak defence for vulnerable populations. It will be weaker in Africa. Endemic poverty, crowded urban slums, limited access to clean water and sanitation, conflict and a weak health infrastructure provide perfect storm conditions for a human crisis of unimaginable dimensions.
Governments across the region are grasping the nettle more decisively than some of their counterparts in the rich world. Screening has been stepped up. Countries are closing airports. South Africa and Zambia are shutting schools. Yet this is a region with permeable borders — and there are almost certainly many unreported cases.
Africa acting alone cannot prevent the spread of coronavirus. The region’s rapidly deteriorating growth prospects, fiscal constraints and limited access to credit markets limit the room for manoeuvre. International support is critical. Yet the response has been piecemeal. Individual donors and philanthropists are supporting important programmes to develop rapid diagnostic kits and vaccines, and to supply equipment. But the current effort will be swamped by the impending health tsunami.
To its credit, the World Bank has moved quickly to mobilise resources, committing $8bn to strengthening health systems in affected countries. That money must be converted with urgency into diagnostic testing kits, medical oxygen supply, protective equipment and training for health workers. But the coronavirus response is also an opportunity to put in place the foundations for the only real defence against pandemic health threats — universal health coverage buttressed by international co-operation.
The WHO is uniquely well-placed to co-ordinate and steer the response. Yet only about one-quarter of the $675m emergency appeal launched last January is funded by donors. That under-investment is the ultimate false economy. In our interdependent world, you can’t beat a global pandemic in your own backyard while letting it take off in a region of a billion people. As even the president of the United States is now discovering no country is an island and viruses don’t carry United States is now discovering, no country is an island — and viruses don t carry
passports.
This article was first published on the Financial Times on March 20, 2020

By Keith Kibirango
Regardless of what the numbers tell us and thoughts we may have regarding infection rates across Africa, we cannot confidently say we will not be as affected as other parts of the world. The low infection rate on the continent could be down to limited international travel, the warmer weather or insufficient testing. It is the lack of knowledge that should fill us with fear and dread.
I tend not to ignore scientists when they produce articles that talk about Africa sitting on a ticking time bomb. The World Health Organisation also calls for African leaders to wake up to a potential crisis.
As of a couple of days ago, Africa had 529 cases, 13 deaths and 41 recovered: with the largest numbers in Egypt, Algeria and South Africa. This is relatively low when compared to other countries like China, Italy and Iran where the death role is in thousands.
My argument is that this is only part of the story.
In all fairness, many African countries have put in place swift and drastic measures to curb the spread of Covid-19. South Africa, Nigeria and Ethiopia have barred travel from high-risk countries like Italy, South Korea, Spain, Germany, France, Switzerland, United States, United Kingdom and China. Kenya, Uganda and Cameroon have shut down schools, restaurants and even reduced the number of people attending burials. Rwanda has filed its capital with portable sinks for hand washing in public areas. However, the devil is in the implementation which is proving to be the hardest bit.
For many African countries, policing the behaviour of their population is terribly difficult. From the crowded cities where people have to go to markets to buy food, travel in cramped public transport and, in most cases, there is no access to water points for hand washing. Poor infrastructure also means that there are some areas where public officials are hamstrung by poor roads to enforce any form of social distancing. It will be next to impossible to stop relatives from burying a dead one, often spending days in a small house in mourning. All this goes against the guidance of how not to behave if we are to limit Covid-19 infections.
In one African country, some folks have been seen to find ways out of a quarantine hotel provided at the airport.
What has this got to do with Africa philanthropy you may ask?
We have had big announcements of support from Bill Gates and Jack Ma who have offered financial support and gifts in kind to fight the spread of COVID-19 on the continent. We are yet to see a similar commitment from African philanthropists who could make a difference in supporting governments that would be overwhelmed by a pandemic.
African governments have limited capacity to tackle the numbers currently seen in Asia, North American and Europe. With over 7,100 multi-millionaires, Africans are not lacking in the capacity to make significant donations to help tackle this pandemic.
Now is the time to address COVID-19 across the continent. We cannot assume immunity, nor can we afford to wait for the treatment phase which is far too expensive in terms of human cost and finance. As the World Health Organisation says, we need to act swiftly and act now. Our best course of action as Africa is prevention, prevention, prevention!
Africa’s philanthropists can help by providing financial assistance that will help strengthen our weak health systems, encourage behavioural change like self-isolation and improved hygiene. This is especially important in crowded spaces like slums, refugee camps and poorer settlements where buying soap may be out of the question for many.
African philanthropists can also use their position to make sure people take the threat of COVID-19 seriously. A message from a respected and influential person on social media can have much more impact than many government directives. By going on social media and encouraging washing of hands, respected African philanthropists can make a huge difference. Like sports personalities and rock stars in the West, these individuals can be so inspiring and are able to amplify the message. Finally any gifts in kind like the use of conference-call facilities and access to space for charities and health workers will help relieve the pressure on national health systems in many African countries, should there be more cases.
In my role as Head of Africa Philanthropy at Save the Children, I believe that together with African philanthropists we can do a lot in supporting our health systems and reaching the most vulnerable in our society. Despite the world focusing more on tackling COVID-19, for many vulnerable African children, there are still huge challenges of malnutrition, illness and lack of adequate protection from abuse. We can ensure that we are better prepared should there be an outbreak while also not compromising other impactful work that saves lives. We have to strive hard to stop COVID-19 from reaching our communities.
This is the time for “Ubuntu” which translates as “humanity towards others” as our way of fighting COVID-19 across Africa by protecting and supporting each other.
This article was first published on Africa Legal on March 20, 2020

As the global leader in child-focused humanitarian response, Save the Children knows that kids are particularly vulnerable during infectious disease outbreaks. For a variety of reasons, including the immediate impacts on their health to social disruptions caused by outbreaks, children can be greatly affected.
The current coronavirus or COVID-19 outbreak has now spread across more than 145 countries/regions worldwide. While the Centers for Disease Control and Prevention (CDC) has noted that most confirmed cases of COVID-19 have occurred in adults[i], it’s important to note that infections in children have been reported as well.
Save the Children’s guidance on how to protect children from coronavirus follows that of the World Health Organization -- practicing good hygiene is the best way to prevent illness. However, there are additional ways in which children can be affected by coronavirus, even if they don’t get sick. For example, we know infectious diseases can disrupt the environments in which children grow and develop. Also, some preventative measures taken by health and medical professionals to control the spread of the disease can present risks to children, including in the area of child protection.
“We know from our work fighting Ebola that children can be at great risk in a health crisis,” said Amy Richmond, Save the Children’s Director of Child Protection in Emergencies. “It is essential to put into place the plans that will ensure children’s health, safety and psychological well-being are the forefront of government and community responses.
Here are 6 things to consider, based on Save the Children’s history of responding to global pandemic threats, about the ways in which children around the world can be affected by coronavirus, even if they don’t get sick.
1. Children’s dependency on adults put them at risk
Children, especially younger ones, are dependent upon their caregivers for meeting their basic needs like food and shelter. If an adult caregiver in a child’s life falls ill, the child’s basic needs could be impacted.
From the start of the Coronavirus outbreak, the World Health Organization emphasized that the best way to avoid spread of the Coronavirus is to keep routine hand washing and good cough etiquette. However, we know that children are less likely to adhere to some basic hygienic practices without adult supervision.
2. Reduced parental supervision can leave children more vulnerable to violence
During infectious disease outbreaks, caregivers may be unable to provide attentive care to their children due to illness, psychological distress, or other reasons. Reduced parental supervision can leave children more vulnerable to violence, exploitation and abuse.
In Yemen during the cholera outbreak in 2017, children who accompanied their sick caregivers to cholera treatment centers were at times left alone to sleep outside on the veranda while their caregivers were admitted for treatment. This unsupervised arrangement exposed children, especially girls, to risks of harassment, sexual violence and abuse.[ii]
3. Disruptions to family income can have immediate and longer-term consequences
Infectious disease outbreaks can have a devastating effect on families by limiting sources of income of family members due to illness, due to the need to care for sick family members, or by increasing household health-related expenses.
During an outbreak of Chikungunya in Orissa, India in 2006, for example, a
study showed that families’ increased health-related expenses threatened their ability to pay for other necessities.[iii]
4. A lapse in education can cause children to feel anxious
Children can perceive time differently to adults, and a few weeks or months out of school may seem like a much longer period of time to them. This means children tend to feel particularly anxious about any period of time they are out of school and the learning and socialization they are missing. They fear they will not be able to catch up and start to worry that the longer schools are closed, the more likely they are to forget what the previously learned.
In Sierra Leone, during the Ebola crisis, children said they felt they were becoming “backward.”
5. Interruptions in social interactions can impact children’s emotional well-being
Beyond the family, children’s relationships with their friends can also be disrupted due to an infectious disease. Children may not be able to play or interact with their friends regularly or at all for long periods of time. Social interactions children have with peers play an important role in children’s social development.
During the Ebola outbreak in Sierra Leone, children reported feeling sad, lonely and lost without the camaraderie of their peers.[iv]
6. At the community level, infectious diseases can disrupt the cultural way of life
Children generally grow and develop within family and friendship circles that are nested within communities. Disruptions to families, friendships and the wider community can have detrimental consequences for children’s well-being, development and their protection.
The SARS outbreak in Singapore in 2003 had a psychological impact on healthy community members, fostered by anxiety and fear of infection.[v] In Tanzania, the impacts of a Rift Valley fever (RVF) outbreak in 2007 included the stigmatization of affected communities for having lost “respect and dignity.”[vi] All of these community-level impacts affect children.
As Save the Children works around the clock to help ensure the health, safety and emotional well-being of children, our teams are providing training and equipment to help reduce the risk of the disease spreading. As with all disease outbreaks, children and families who have limited access to health care or clean water are the most vulnerable.

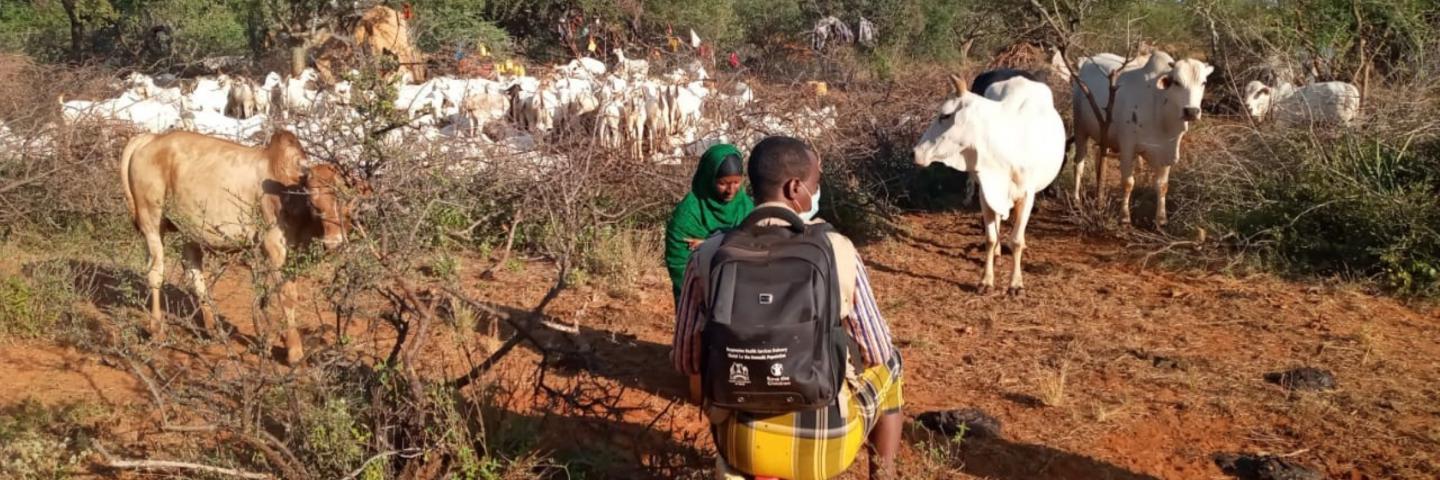
By Ahmed Osman
At about 10 am amid the searing heat and dust Ali Adan, 42, a Community Health Volunteer (CHV) is doing his routine visit to a homestead. This homestead however is not ordinary. It is a nomadic community unit made up of 30 households. The community units are the lowest level health service delivery structures with a population of up to 5, 000 persons served by CHVs. Adan has been trained by Save the Children through the support of the Nomadic Health Project (NHP) funded by BMGF to be able to provide an array of services to nomadic communities. Nomadic communities in North Eastern Kenya are underserved by health services because they are constantly on the move usually in remote areas in search of pasture and water for their animals away from health and social services. Due to these reasons the area records high maternal mortality and child deaths. According to UNFPA Mandera ranks as having the highest maternal mortality rate in the country with 3,795 per100, 000 live birth while Wajir has 1,683 maternal deaths per 10,000 live birth.
Adan is among 11 other CHVs that have been trained to treat minor ailments and injuries such as diarrhea. He refers pregnant women for antenatal services and children for vaccinations. He is also tasked to provide the nomadic population with health education. Before he was trained no one in his community had basic health knowledge and common childhood illness like diarrhea was rampant. Consequently child immunization was low and many mothers delivered at home.
The project run by Save the Children aims to improve access to health services especially access to reproductive health services and family planning to the Nomads who constitute 60% of the population in Wajir and Mandera counties according to the Kenya National Households Survey 2009. The project formed 15 nomadic community units in Wajir and Mandera where CHVs were trained to deliver basic health services to nomadic communities while they are on the move. The services provided to these
community units include treatments of minor ailments, nutritional screening, disease surveillance, health education, immunisation and referral. So far over 37,000 nomadic children have received various health services through the project.
“The incidence of diarrhoea among children under five years old has reduced dramatically and today many nomadic children can get vaccines and deworming medicines for the first time in their life time while on the move,” said Aden Abdullahi.
COVID-19 Interventions
There are currently 16 confirmed cases of COVID-19 in Wajir County. Abdullahi said that CHVs in the community units remain useful and continue to provide health information on the virus to the nomadic populations. “They are supporting contact tracing and linking of suspected to health facilities. They also play a critical role of decongesting health facilities by providing essential services at community level,” he added.